Maxwell Obubu1, Nkata Chuku2, Alozie Ananaba3, Rodio Diallo4, Emmanuel Sambo5, Oluwatosin Kolade6, Tolulope Oyekanmi7, Kehinde Olaosebikan8, Oluwafemi Serrano9
1Health Systems Consult Limited (HSCL), No. 856 Olu-Awotesu Street, Jabi, 900101, Abuja, Federal Capital Territory, Nigeria
2Bill and Melinda Gates Foundation, No. 43 Agadez Cres, Wuse 2, 904101, Abuja, Federal Capital Territory, Nigeria
3Head of Operations, Lagos State Health Management Agency (LASHMA), No. 17 Kafi Street, Alausa Ikeja, 101233, Lagos State, Nigeria
Correspondence: Maxwell Obubu, Health Systems Consult Limited (HSCL), No. 856 Olu-Awotesu Street, Jabi, 900101, Abuja, Federal Capital Territory, Nigeria, Tel +2348031951850
Citation: Obubu M, Chuku N, Ananaba A, et al. Choices and availability of family planning services: evidence from census-based health facility assessment data in Bauchi state, Nigeria. MOJ Public Health. 2023;12(1):61-65.
Abstract
Background: Controlling family planning (FP) has long been the goal of most nations and cultures. FP aims to keep the population under control while also improving living conditions. Many countries, especially the developing ones, which Nigeria is among, face the challenge of dealing with overpopulation due to high fertility rates. FP is considered a veritable way of dealing with high fertility problems. The present study assesses the choices and availability of FP services in Bauchi state health facilities.
Methods: This study leveraged Noi Polls census data on Health Facility Assessment for Bauchi state. We conducted a descriptive analysis and analyzed the primary health facility assessment data using counts and percentages.
Result: Findings of the study revealed that 80% of the health facilities studied in Bauchi State offer FP services. 91.2% and 77% of the facilities in the urban and rural areas, respectively, offer FP services. This translates to 8.8% and 23% of health facilities in urban and rural areas, respectively, not offering FP services. Based on proportions, assessing the facilities that offer FP by ownership shows that public health facilities are more into FP services (80%) compared to the private-for-profit (80%) health facilities and facilities owned by NGOs and faith-based organizations (83.3%). By facility level of care, 87.5% of secondary healthcare facilities in Bauchi State offer FP services compared to primary healthcare facilities (79.5%). FP services provided in the studied facilities include counseling, contraceptive injectables, oral contraceptive pills, male and female condoms, implants, Intra-Uterine Contraceptive Devices IUCD, sterilization methods, and natural/traditional methods.
Conclusion: Considering that over 80% of health facilities considered in this study locates in rural Bauchi state, with over 22% not offering FP clearly shows a gap that the government must address. The distribution of FP services across the state's local government areas is inequitable as some local governments have more health facilities offering the services than others, thus giving residents in those areas a higher chance of benefitting from those services.
Keywords: family planning, contraceptive methods, census-based data, health facility assessment, FP services
Background
Nigeria is Africa's most populated and the world's seventh-largest country, with over 200 million people.1 Nigeria's fertility rates have remained relatively high for several years.2 As noted by the Nigeria Demographic and Health Survey in 2014, the average total fertility rate in Nigeria was 6.1 births per woman, with up to 9 in Northern Nigeria.2 Following Nigeria's fertility trends, studies revealed that contemporary contraception use has remained low, with only about 15% of Nigerian women using it as of 2014.2
Even though Nigeria's FP program began many years ago, it has one of Africa's lowest contraceptive prevalence rates (CPR) at 17% in 2018.3 In 2014, as reported by the Nigeria Demographic and Health Survey (NDHS), the overall contraceptive prevalence rate (CPR) among all Nigerian women was 15%, with a further 16% of unmet needs.4 As a result, the country's fertility rate has remained high. The country's Northwestern region had a statistic of 5.3 births per woman in 2018.5 Bauchi State has the country's highest total fertility rate of 7.0.5 These findings highlight the difficulties in achieving universal health coverage and ensuring long-term healthcare delivery in Nigeria.
Despite the high fertility rate in Nigeria, factors contributing to it are still not given the needed attention. According to Aransiola, et al.,6 these factors are religion, poor accessibility to FP services, or a complete lack of it in some cases, cultural hurdles such as patriarchy, and a lack of male involvement in FP. Despite a high birth rate and unmet needs in Nigeria, FP is still underutilized among women.7,8 The rapidly growing population caused by the high birth rate impedes the rapid improvement of human welfare in developing countries.6
Based on the foregoing, community use of FP services is low in Nigeria, as evidenced by the 2018 Nigeria Demographic and Health Survey.3 Most married Nigerian women do not plan to use modern FP methods, according to the survey. Therefore, this study investigates the choices and availability of FP services in healthcare facilities in Bauchi State, Nigeria.
Methodology
The study leveraged primary data collected on health facilities assessment in Bauchi State by NoIPolls. HSCL developed a quantitative list of health facilities using information from the State Ministry of Health (SMOH) and the State Primary Health Care Development Agency (SPHCDA). The list served as a sample frame for health facilities in Bauchi State. The sample frame consisted of 1,108 health facilities, and a census approach was adopted. The data collection method used was Computer Assisted Telephone Interview (CATI). Health facilities' target respondents (Chief Medical Directors and Medical Directors) were interviewed through the telephone using Questionnaire Processing Software for Market Research (QPSMR). The software allows for custom logic, skipping or filtering of questions, data entry error control, quality control checks, specific quotas, and overall project management. The telephone interview call protocol specifies that each health facility in the sample frame is assessed six times through an interview before the facility falls in the category of unsuccessful calls. One thousand one hundred eight (1,108) health facilities were assessed with 438 uncompleted calls/interviews. In total, there were 670 completed interviews for the survey. The final health facility assessment dataset contains information on Facility Ownership, Facility level of Care, Accrediting body, Human Resources for Health, Basic Medical & Infection Prevention Equipment, Infrastructure, Available Services, Health Insurance Coverage, Medicines & Commodities, Financial Management Systems, Clinical Governance, and Covid-19 Response.9
Statistical method and results
The method of analysis employed in the study is descriptive statistics. We used percentages to assess the distribution of facilities and personnel distributions across the state. Statistical Package for Social Sciences (SPSS) was used in carrying out the analysis.
Table 1 shows the distribution of health facilities by LGA in Bauchi. Ninety-seven (97) healthcare facilities representing 14.5% of the total health facilities for this study were assessed from Bauchi LGA, and two healthcare facilities representing 0.3% of the total facilities included in this study were assessed from Zaki LGA Figure 1.
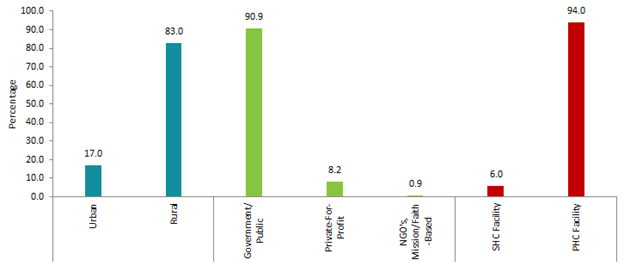
Figure 1 Percentage Distribution of Health Facilities Assessed by 'Locality,' 'Facility Ownership Type,' and 'Facility Level of Care'.
| LGA | Count | Percentage |
| Alkaleri | 45 | 6.7 |
| Bauchi | 97 | 14.5 |
| Bogoro | 23 | 3.4 |
| Damban | 32 | 4.8 |
| Darazo | 34 | 5.1 |
| Dass | 29 | 4.3 |
| Gamawa | 38 | 5.7 |
| Ganjuwa | 51 | 7.6 |
| Giade | 22 | 3.3 |
| Itas/Gadau | 20 | 3.0 |
| Jama'are | 23 | 3.4 |
| Katagum | 33 | 4.9 |
| Kirfi | 26 | 3.9 |
| Misau | 23 | 3.4 |
| Ningi | 33 | 4.9 |
| Shira | 24 | 3.6 |
| Tafawa-Balewa | 47 | 7.0 |
| Toro | 53 | 7.9 |
| Warji | 15 | 2.2 |
| Zaki | 2 | 0.3 |
| Total | 670 | 100.0 |
Table 1: Distribution of Health Facilities Assessed (by Local Government Areas (LGAs))
Table 2 presents the total percentage of facilities offering FP services in Bauchi State, and we distributed the result by facility ownership type, level of care, and locality. Glaringly, 80% of the studied facilities offer FP services to clients, while 20% do not. 91.2% of the health facilities in the state's urban areas provide FP services, and 77.7% of the rural facilities also offer the same services. The percentage of government/public facilities offering FP services is 80% and is the same for private-for-profit facilities. In contrast, NGOs, Mission/Faith-based health facilities record 83.3% offering FP services. The result further shows that 87.5% of secondary healthcare facilities and 79.5% of primary healthcare facilities in the state offer FP services.
| Total | Ownership Type | Facility's Level of Care | Facility's Locality | |||||
| Government/Public | Private-For-Profit | Others (NGOs, Mission/Faith-Based) | SHC Facility | PHC Facility | Urban | Rural | ||
| Yes | 80.0 | 80.0 | 80.0 | 83.3 | 87.5 | 79.5 | 91.2 | 77.7 |
| No | 20.0 | 20.0 | 20.0 | 16.7 | 12.5 | 20.5 | 8.8 | 22.3 |
Table 2 The percentage of facilities providing FP services (by Ownership type, level of care, and locality)
Table 3 depicts the distribution of health facilities offering FP services in the state and the FP services distributed by the local government. All the facilities (100%) surveyed in Dass LGA offer FP services; this is closely followed by Bogoro local government with 95.7%, and Tafawa-Balewa, Jama'are, and Katagum with 91.5%, 91.3%, and 90.9%, respectively. However, Zaki LGA has the least number of healthcare facilities in Bachi state, with 50% of facilities surveyed offering FP services. Bauchi is the local government with the highest number of facilities surveyed (95); only 83.5% of these facilities (i.e., 81) offer FP services. We also examined the different FP services provided by healthcare facilities in local government areas in Bauchi state and presented our findings in Table 3.
| LGA | Total number of Facilities | % of Facilities offering FP services | % of Available FP services | |||||||||
| Count | Count | % | FP counseling | Contraceptive Injectables | Oral Contraceptive pills | Intra Uterine Contraceptive Devices IUCD | Provision of implants | Provision of condoms (male) | Provision of condoms (female) | Sterilization | Natural/Traditional Methods (Calendar, Cycle Beads, Withdrawals) | |
| Alkaleri | 45 | 34 | 75.6 | 100 | 100 | 97.1 | 35.3 | 67.6 | 91.2 | 58.8 | 20.6 | 11.8 |
| Bauchi | 97 | 81 | 83.5 | 100 | 95.1 | 95.1 | 65.4 | 84 | 85.2 | 76.5 | 32.1 | 13.6 |
| Bogoro | 23 | 22 | 95.7 | 100 | 95.5 | 95.5 | 9.1 | 68.2 | 95.5 | 81.8 | 4.5 | 9.1 |
| Damban | 32 | 20 | 62.5 | 95 | 95 | 95 | 25 | 85 | 95 | 75 | 10 | 5 |
| Darazo | 34 | 20 | 58.8 | 100 | 90 | 85 | 55 | 80 | 70 | 65 | 15 | 20 |
| Dass | 29 | 29 | 100.0 | 100 | 100 | 100 | 62.1 | 82.8 | 100 | 75.9 | 17.2 | ... |
| Gamawa | 38 | 32 | 84.2 | 100 | 96.9 | 93.8 | 65.6 | 93.8 | 93.8 | 78.1 | 18.8 | 9.4 |
| Ganjuwa | 51 | 35 | 68.6 | 97.1 | 91.4 | 85.7 | 20 | 71.4 | 68.6 | 48.6 | 11.4 | ... |
| Giade | 22 | 18 | 81.8 | 100 | 100 | 100 | 38.9 | 72.2 | 88.9 | 83.3 | 44.4 | 22.2 |
| Itas/Gadau | 20 | 14 | 70.0 | 92.9 | 92.9 | 92.9 | 50 | 85.7 | 78.6 | 42.9 | 21.4 | 7.1 |
| Jama'are | 23 | 21 | 91.3 | 100 | 95.2 | 95.2 | 28.6 | 85.7 | 95.2 | 71.4 | 9.5 | ... |
| Katagum | 33 | 30 | 90.9 | 100 | 100 | 100 | 60 | 100 | 96.7 | 90 | 26.7 | 10 |
| Kirfi | 26 | 23 | 88.5 | 100 | 100 | 100 | 56.5 | 91.3 | 100 | 65.2 | 39.1 | 8.7 |
| Misau | 23 | 18 | 78.3 | 100 | 100 | 94.4 | 55.6 | 94.4 | 100 | 94.4 | 33.3 | 11.1 |
| Ningi | 33 | 25 | 75.8 | 100 | 92 | 96 | 72 | 100 | 80 | 76 | 28 | 4 |
| Shira | 24 | 17 | 70.8 | 100 | 94.1 | 100 | 29.4 | 76.5 | 100 | 70.6 | 17.6 | ... |
| Tafawa-Balewa | 47 | 43 | 91.5 | 100 | 97.7 | 97.7 | 18.6 | 86 | 86 | 55.8 | 14 | 11.6 |
| Toro | 53 | 42 | 79.2 | 100 | 100 | 97.6 | 45.2 | 81 | 95.2 | 73.8 | 28.6 | 9.5 |
| Warji | 15 | 11 | 73.3 | 100 | 90.9 | 81.8 | 54.5 | 81.8 | 81.8 | 63.6 | 18.2 | 9.1 |
| Zaki | 2 | 1 | 50.0 | 100 | 100 | 100 | ... | ... | 100 | 100 | 100 | ... |
Table 3 Percentage Distribution of Facilities offering FP services and the various FP services offered (across the Local Government Area)
Table 4 shows the different FP services offered by the health facilities in Bauchi State. The result shows that the service provided mainly by the health facilities is counseling, which 79.6% of the study provided. This is followed by contraceptive injectable provided by 77.2% of the facilities. Only 7.2% of the studied facilities include natural/traditional FP methods in their list of services. Another FP method that is not widely provided in Bauchi state is sterilization, which is provided by 18.1% of the studied facilities. Assessing the FP services by the local government shows that all the studied healthcare facilities in the state offer FP counseling except Damban, Ganjuwa, and Itas/Gadau local government areas, with 95%, 97.1%, and 92.9%, respectively, of the facilities offering FP counseling.
| Services | Total | Facility's Level of Care | Facility Ownership Type | Facility Locality | ||||
| SHC Facility | PHC Facility | Government/Public | Private-For-Profit | Others (NGOs, Mission/Faith-Based) | Rural | Urban | ||
| FP counseling | 79.6 | 100.0 | 99.4 | 99.4 | 100.0 | 100.0 | 77.2 | 91.2 |
| Provision of contraceptive injectables | 77.2 | 94.3 | 96.6 | 96.9 | 93.2 | 80.0 | 75.0 | 87.7 |
| Provision of oral contraceptives pills | 76.3 | 100.0 | 95.0 | 95.5 | 95.5 | 80.0 | 73.9 | 87.7 |
| Provision of condoms (male) | 71.3 | 80.0 | 89.8 | 90.3 | 77.3 | 80.0 | 69.1 | 82.5 |
| Provision of implants | 66.7 | 88.6 | 83.0 | 84.2 | 75.0 | 80.0 | 64.4 | 78.1 |
| Provision of condoms (female) | 56.9 | 54.3 | 72.3 | 72.9 | 50.0 | 80.0 | 55.0 | 65.8 |
| Provision of Intra-Uterine Contraceptive Devices IUCD | 36.7 | 80.0 | 43.5 | 45.2 | 56.8 | 20.0 | 32.6 | 57.0 |
| Sterilization methods | 18.1 | 54.3 | 20.4 | 20.3 | 50.0 | ... | 15.8 | 28.9 |
| Natural/Traditional Methods (Calender, Circle Beads, Withdrawal etc.) | 7.2 | 17.1 | 8.4 | 7.4 | 20.5 | 60.0 | 6.1 | 12.3 |
Table 4 Percentage Distribution of Facilities offering FP services (classification by Ownership type, Level of Care, and Locality)
Discussion of findings
More than three decades ago, the Federal Government of Nigeria, in a bit to address the growing population concern, launched the National Population Policy for development, unity, progress, and self-reliance, in 1988, with a critical goal of lowering fertility rates through FP techniques, among other factors.10 According to section 4.2.3 of the policy, one of the goals is to make FP tools and services available to all couples and people at an affordable cost as soon as possible to control their reproductive health. One of the techniques for doing this was to educate and inspire the general public about FP's health, social, and demographic benefits at the grassroots level.10
The Nigerian government's first significant health program with an FP component was the Family Health Services Project.11 Until developing challenges like HIV/AIDS, gender inequality, and poverty necessitated reconsideration, this scheme remained one of Nigeria's only major FP initiatives.11 The above-mentioned goal is similar to public fertility-reduction programs, aiming to minimize the demand for children, postpone childbearing, and maximize contraceptive use.12
Again, the Federal Ministry of Health of Nigeria (FMOH) and the US Agency for International Development (USAID) collaborated on a five-year project aimed at improving contraceptive prevalence across the country by making FP information and services widely available at reasonable costs in both the private and public sectors.13 Although ten major FP programs have been implemented in various parts of the country since the first project, Nigeria's fertility rate has remained high despite these interventions.2,14
Controlling human fertility has long been a goal of most nations and cultures. In other words, fertility control, or FP aims to keep the population under control while improving living conditions.15 Since 1960, the population of Bauchi has grown from one million in 1960 to about 7.3 million in 2017.16 While the Bauchi state government recognizes the need to improve access to critical resources such as education, healthcare, and job opportunities, more investment in FP is required to help the state avoid the adverse implications of the rapidly growing population.16 As defined by. Cleland, et al.,17 FP services are "educative, comprehensive medical or social activities that allow people to select the number and spacing of their children and how they choose to do it."17 Similarly, they noted that preconception care and counseling for planning pregnancies must be widely adopted, necessitating the availability of FP services. FP services can potentially increase the use of preconception care, which is generally underutilized. Preconception care during the reproductive years is contingent on the woman and man planning their conceptions, not only in terms of timing but also in health-related aspects that would maximize their chances for a successful pregnancy and healthy baby.17
The value of FP in any community cannot be overstated. FP practices can improve maternal and child health by avoiding sexually transmitted illnesses (STIs) and unplanned and early pregnancies.18,19 FP practices have improved people's lives through increased national security and community financial resources.20 The United Nations has highlighted increasing and maintaining the usage of FP services as one of its critical strategic agenda emphasis areas to achieve sustainable development goals (SDGs). By investing in various FP services initiatives at national and community levels worldwide, the United Nations hopes to provide universal access to sexual and reproductive health (SRH) services, such as FP methods, information, and education, by 2030.21
However, women's age, education, and socio-economic level in Nigeria are significant determinants of contraceptive use.22 Nigerian women with higher education are more likely to plan their families, have fewer children, have greater access to health care, and lower infant mortality.22 Similarly, Osemwenkha23 stated that contraceptive users enjoy a higher quality of life, a higher social position, and more liberty. This link was also underlined in a Nigerian study, which found that contraceptive use can significantly lower fertility and, as a result, improve the health of mothers and children.24 Despite a high degree of understanding and approval of FP,24 pointed out that the socio-cultural impact of husbands' awareness of FP on wives and daughters impedes the utilization of current FP techniques. Hence, there is a need to improve awareness about FP's availability and its benefits in terms of child spacing, family health, and, eventually, population management and societal health.25
Male methods, such as condoms and sterilization, have been introduced into FP efforts in many parts of the world. Still, male adoption of these methods has been shallow, partially due to perceived conflict with traditional culture, patriarchal norms, notions of maleness, and religion.26 Similarly, the price and availability of substitutes, location of settlement (rural or urban), the presence of health insurance, age, education, indirect consumer costs, household/community preferences, community attitudes, and norms make it difficult for people to embrace and use family services.27 Other factors influencing the use of FP services, as noted by, Casterline et al.,28 include the overall cost and availability of contraceptive commodities, transportation, and provider fees for contraceptives and healthcare services, fear of side effects, spousal approval, culture, and religion.
A country's population is a function of its fertility rate. The higher the fertility rate, the higher the population. Many countries, especially the developing ones, of which Nigeria is a part, now face the challenge of dealing with overpopulation due to high fertility rates. FP is a veritable way of dealing with high fertility problems.20 The study's findings revealed that 80% of the health facilities studied in Bauchi State offer FP services. This shows that Bauchi State has put measures in place to tackle the high fertility rate in the state.5 via FP.
More attention is given to health facilities in urban areas of the state, as 91.2% offer FP services. In comparison, 77.7% of the facilities in rural areas offer FP services, meaning that 22.3% do not offer such services. This high availability of FP services gives the state's urban residents a higher chance to assess these services than those in rural areas, as evidenced in the study by, Duru, et al.,7 By proportions, assessing the facilities that offer FP services by facility ownership, the result shows that public health facilities are more into FP services (80%) followed by private-for-profit (80%) health facilities, and then, the NGOs and faith-based organizations (83.3%). Considering the number of secondary healthcare facilities in this study, we cannot out rightly say that they are more concerned with FP services than primary healthcare facilities despite having a higher percentage (87.5%). However, Onoja, et al.,18 noted that the availability of FP services in healthcare facilities is subject to the availability of trained human resources for health (HRH) personnel for those services. HRH personnel are found more in secondary healthcare facilities, which may sway more clients to seek FP services.18
Facilities offering FP services in Bauchi State are not evenly distributed across the local government area, as shown in Table 3. Findings revealed that all the studied facilities in Dass local government offer FP services, followed by Bogoro (95.7%). The least is Zaki local government area, with 50% of the studied facilities offering FP services. Services such as the implant, Provision of Intra-Uterine Contraceptive Devices, and Natural/Traditional Methods are not offered in the two health facilities in Zaki local government area. Findings revealed that the least provided services across all the local government areas are natural/traditional and sterilization methods. This implies that these methods are not widely used.19 Since the trained personnel have no solid recommendations for those methods. The FP services offered most in the studied facilities are contraceptive injectable, oral contraceptive pills, and male condoms, which again collaborate with.19
The FP services provided in the studied facilities are counseling, provision of contraceptive injectables, oral contraceptives pills, provision of male and female condoms, implants, provision of Intra-Uterine Contraceptive Devices IUCD, sterilization methods, and natural/traditional methods (Calendar, Circle Beads, Withdrawal), as also evidenced in Duru, et al.,7 Findings revealed that the service offered most is counseling by 79.6% of the studied facilities, followed by contraceptive injectables (77.2%), and the least is the traditional/natural methods. The traditional method was also the least used by Olaleye, et al.,19 and one of the least by Duru, et al.,7 Most of the studied facilities in Bauchi State offer FP services, yet the fertility rate in the state is very high compared to other states.5 The result shows that residents in the state are not accessing the available FP services.
Conclusion
The importance of FP to maternal and child health and population control cannot be emphasized. The usage of these services depends mainly on their availability in the healthcare facilities available in the localities. Considering the number of healthcare facilities offering FP services in Bauchi State, it is safe to say that the service has been made available to the people of Bauchi State. Although the services are provided more in the urban areas, the facilities in the rural areas providing FP services are considerably high. The distribution of FP services across the state's local government areas is inequitable as some local governments have more facilities offering the services than others. This means that the people in the local government areas with more facilities offering FP services have a higher chance of befitting from those services than others. Public Healthcare facilities are involved more in FP services than private-for-profit-owned facilities and NGOs/faith-based organizations when we consider the proportion of facilities considered in the study. FP methods provided by more than 60% of the health facilities in Bauchi State include counseling, contraceptive injectables, oral contraceptive pills, male condoms, and implants. In comparison, the least recommended methods provided by less than 20% of the facilities are sterilization and natural/traditional methods.
Acknowledgments
None.
Conflicts of interest
The authors declare that there is no conflict of interest.
References
- Definition of Regions. World Population Prospects Revision: United Nations Department of Economic and Social Affairs, Population Division, Population Estimates and Projections Section. 2019.
- NPC & ICF International. Nigeria Demographic and Health Survey. USAID. 2014.
- NPC & ICF International. Nigeria Demographic and Health Survey, Abuja, Nigeria, and Rockville, Maryland, USA. 2018;43–162.
- Federal Ministry of Health (FMOH). Nigeria family planning blueprint (Scale-up plan). 2014.
- National Population Commission (NPC). Population Policy. 2018.
- Aransiola JO, Akinyemi AI, Fatusi AO. Women's perceptions and reflections of male partners and couple dynamics in family planning adoption in selected urban slums in Nigeria: A qualitative exploration. BMC Public Health. 2014;14:869.
- Duru CB, Nnebue CC, Iwu AC, et al. Utilization of family planning services among women of reproductive age in urban and rural communities of Imo State, Nigeria: a comparative study. AJOL. 2018;6(1):11–26.
- Odusina E, Ayotunde T, Kunnuji M, et al. Fertility preferences among couples in Nigeria: a cross sectional study. Reproductive Health. 2020;17(92).
- Obubu M, Chukwu N, Ananaba A, et al. Bauchi State Health Facility Assessment Tool. Figshare. 2023.
- Federal Government of Nigeria. National Policy on Population for Development, Unity, Progress, and Self-Reliance., Federal Ministry of Health, (OCoLC) 654739014: Lagos, Nigeria: Dept. of Population Activities. 1988.
- Okpala A. Nigerian population growth and its implications for economic development. Scandinavian Journal of Development Alternatives. 1990;9(4):63–77.
- Mberu B. Fertility Levels and Family Planning in Rural Nigeria: An Assessment of Akokwa Community, Imo State. Department of Sociology, University of Ibadan. Volume Unpublished MA Dissertation. 1990. p. 3–6.
- Pathfinders International. Nigeria Family Health Services. 1993. p. 1–5.
- World Bank. World Development Indicators. 2017.
- Omolase C, Faturoti S, Omolase B. Awareness of Family Planning Amongst Antenatal Patients in a Nigerian Community: An Exploratory Study. Annals of Ibadan Postgraduate Medicine. 2009;7(1):36–39.
- Health Policy Plus. Nigeria Population and Development: Bauchi State (Fact sheet). Abuja, Nigeria. 2017.
- Cleland J, Bernstein S, Ezeh A, et al. Family planning: the unfinished agenda. Lancet. 2006;368(9549):1810–1827.
- Onoja A, Sanni F, Akogu S. Assessing the Current States of Logistics Management and Training on Family Planning Services in Nigerian Healthcare Facilities. International Journal of Tropical Disease. 2021;42(6):27–36.
- Olaleye A, Akintaye A, Adewoyin Y, et al. Utilization of family planning services in a Nigerian tertiary Hospital: A six year review. Trop J Obstet Gynaecol. 2014;31(2):7–15.
- Cates W. Family planning: the essential link to achieving all eight millennium development goals. Contraception. 2010;81(6):460–461.
- Starbird E, Norton M, Marcus R. Investing in family planning: key to achieving the sustainable development goals. Global Health Sciences Practice. 2016;4(2):191–210.
- Federal Office of Statistics. Lagos: Federal Office of Statistics. National demographic and health survey (NDHS). 2003.
- Osemwenkha S. Gender Issues in Contraceptive Use among Educated Women in Edo State, Nigeria. African Health Sciences. 2004;4(1):40–49.
- Onwuzurike B, Uzochukwu B. Knowledge, attitude and practice of family planning amongst women in a high density low income urban of Enugu, Nigeria. African Journal Reproductive of Health. 2001;5(2):83–89.
- Ijadunola M, Abiona TC, Ijadunola KT, et al. Male involvement in family planning decision making in Ile-Ife, Osun State, Nigeria. Afr J Reprod Health. 2010;14(4 Spec no.):43–50.
- Seltzer J. The origins and evolution of family planning programs in developing countries. Rand. 2000.
- Helman C. Doctor-patient interactions. In: CG Helman editor. Culture, health and illness (4th edn). London: Arnold. 2001. p. 79–107.
- Casterline J, Sinding S. Unmet need for family planning in developing countries and implications for population policy. Population Development Review Journal. 2000;26(4):691–723.


